
What is Prostate Cancer?
Prostate cancer is a disease in which malignant (cancer) cells form in the tissues of the prostate.
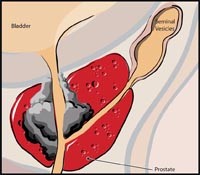
The prostate is a gland in the male reproductive system located just below the bladder and in front of the rectum. It is about the size of a walnut and surrounds the urethra (the tube that empties urine from the bladder). The prostate gland produces fluid that is one of the components of semen.1
Prostate cancer is among the most common cancers diagnosed in men. In the US, one in six men will be diagnosed in his lifetimes.2 While no one will say facing prostate cancer is easy, the good news is with increased awareness and screening, more men are diagnosed early. That means most cancers are found while still localized in the prostate before the cancer has spread.
Statistics
Prostate cancer is the most common non-skin malignancy in men3 and is responsible for more deaths than any other cancer, except for lung cancer. However, microscopic evidence of prostate cancer is found during autopsies in many if not most men.
The American Cancer Society (ACS) estimated that about 186,320 new cases of prostate cancer were diagnosed in the United States during 2008. About 1 man in 6 will be diagnosed with prostate cancer during his lifetime, but only 1 man in 34 will die of it. A little over 1.8 million men in the United States are survivors of prostate cancer.4
Prognosis & Treatment
Treatment options and prognosis depend on the stage of the cancer, the Gleason score5, and the patient's age and general health.
With greater public awareness, early detection is on the rise and mortality rates are declining.
Additionally, new advances in medical technology are enabling cancer patients to return to active and productive lives after their treatment.
Treatment Options
When prostate cancer is believed to be localized, there are five common treatment options available to a patient:
1. Removal of the cancerous prostate (radical prostatectomy)
For localized prostate cancer, radical prostatectomy (removal of the prostate gland and some tissue around it) is considered the definitive way to treat the cancer, byremovingit. An estimated 91% of prostate cancer cases diagnosed in the U.S. are localized, which means many men are potential candidates for cancer removal. But, patients should discuss the advantages and disadvantages of each treatment approach with their doctor.
Surgically removing the cancerous prostate lets your doctor see how aggressive the tumor is and whether it has spread. This step can be critical since 35% of tumors are undergraded to a clinically significant extent. That means the cancer is more aggressive than the pre-surgery assessment and biopsy results indicated.8
Choosing surgery over radiation can make it easier for your doctor to detect a cancer recurrence, through careful PSA monitoring, after a radical prostatectomy than after radiation therapy.9 It can also help preserve your options if your cancer should return. After radiation therapy, there may be damage to the tissue surrounding the prostate. If you have tissue damage, nerve-sparing surgery may no longer be an option if your cancer returns. But, radiation usually remains an option for patients who have had surgical treatment of their prostate cancer.10
With any cancer treatment, the first priority is survival. Several large studies suggest there is a greater chance of long-term survival for patients undergoing surgery over other potential treatments. Patients undergoing radical prostatectomy had a 40% lower risk of death from prostate cancer than radiation patients 15 years after treatment.11 (According to a study of 3,159 men adjusted for age at diagnosis, race, socioeconomic status, Gleason score, biopsy grade of tumor and year of diagnosis.)
da Vinci® Prostatectomy
da Vinci® Prostatectomy is the #1 choice for treatment of localized prostate cancer in the United States
Thanks to a breakthrough surgical technology, surgeons now widely offer a minimally invasive option for prostatectomy, the da Vinci® Prostatectomy.
Imagine major surgery performed through the smallest of incisions. Imagine having the benefits of a definitive treatment but with the potential for significantly less pain, a shorter hospital stay, faster return to normal daily activities - as well as the potential for better clinical outcomes.
In prostate cancer treatment, millimeters matter. Nerve fibers and blood vessels are attached to the prostate gland. To spare these nerves, they must be delicately and precisely separated from the prostate before its removal. Surgeons use the precision, vision and control provided by da Vinci® to assist them in removal of the cancerous prostate while preserving important nerves and blood vessels.
In terms of cancer control, in several large published studies, da Vinci® Prostatectomy has shown equal or lower rates of positive surgical margins (meaning margins with cancer cells left behind) than large studies of other forms of surgery.
Urinary continence and sexual function after treatment are also of concern for prostate cancer patients. Studies show patients who undergo a da Vinci® Prostatectomy may experience a faster return of urinary continence following surgery and lower rates of urinary pain than radiation (brachytherapy) patients. Several studies also show patients who are potent prior to surgery recover their sexual function (defined as an erection for intercourse) within a year following da Vinci Surgery. Talk to your surgeon about reasonable expectations for recovery of sexual function and a rehabilitation program that may include exercises and drug therapy.
It is important to know that da Vinci Surgery does not place a robot at the controls; your surgeon is always in control of every aspect of the surgery with the assistance of the da Vinci robotic surgical systemplatform.
2. Radiation of the cancerous prostate, through either external radiation or radioactive seed implants (radiation therapy or brachytherapy, respectively)
Radiation therapy uses high-energy x-rays, either beamed from a machine or emitted by radioactive seeds implanted in the prostate, to kill cancer cells. When prostate cancer is localized, radiation therapy serves as an alternative to surgery. External beam radiation therapy is also commonly used to treat men with regional disease, whose cancers have spread too widely in the pelvis to be removed surgically, but who have no evidence of spreading to the lymph nodes. In men with advanced disease, radiation therapy can help to shrink tumors and relieve pain.
It is important to be aware that radiation can cause long-term damage to the nerves and important structures involved in sexual function. Many patients undergoing brachytherapy or external beam radiation treatment develop erectile dysfunction (as many as 50% in several studies.) 12, 13 Many radiation patients are also placed on hormone therapy, which has an immediate negative impact on sexual function.
3. Freezing of the cancerous prostate (Cryotherapy)
C ryosurgery uses liquid nitrogen to freeze and kill prostate cancer cells. The doctor places needles in preselected locations in the prostate gland. The needle tracks are dilated for the thin metal cryo probes to be inserted through the skin of the perineum into the prostate. Liquid nitrogen in the cryo probes forms an ice ball that freezes the prostate cancer cells; as the cells thaw, they rupture. The procedure takes about 2 hours, requires anesthesia (either general or spinal), and requires 1 or 2 days in the hospital.14
4. Hormonal therapy, which is non-curative and often done in conjunction with radiation therapy or cryotherapy
Hormonal therapy combats prostate cancer by cutting off the supply of male hormones (androgens) such as testosterone that encourage prostate cancer growth. Hormonal control can be achieved by surgery to remove the testicles (the main source of testosterone) or by drugs.
Hormonal therapy targets cancer that has spread beyond the prostate gland and is thus beyond the reach of local treatments such as surgery or radiation therapy. Hormonal therapy is also helpful in alleviating the painful and distressing symptoms of advanced disease. Further, it is being investigated as a way to arrest cancer before it has a chance to metastasize. Although hormonal therapy cannot cure, it will usually shrink or halt the advance of disease, often for years.15
5. Observation (watchful waiting)
Watchful waiting refers to closely monitoring a patient's condition without giving any treatment until symptoms appear or change. This is usually used in older men with other medical problems and early-stage disease. Watchful waiting is based on the premise that localized prostate cancers may advance so slowly that they are unlikely to cause men?especially older men?any problems during their lifetimes. 17 Some men who opt for watchful waiting, also known as "observation" or "surveillance," have no active treatment unless symptoms appear. They are often asked to schedule regular medical checkups and to report any new symptoms to the doctor immediately.
Experimental / Out-of-Country Treatments
When faced with serious illness, many people explore alternative or experimental treatment options with the goal of easing their symptoms and controlling or eliminating the disease.
A treatment option for prostate cancer currently available outside the United States is High-Intensity Focused Ultrasound (HIFU). HIFU treatment uses the principle of ultrasound energy to destroy cancer cells. To treat prostate cancer, t he energy is delivered to the patient using a transrectal probe under general or regional anaesthesia. Current studies show HIFU has significant complication rates and failure rates in effectively treating cancer in both initial and recurrent prostate cancer cases. As a result, some leading urologists have suspended their use of HIFU pending further evidence of its safety and effectiveness.16
Discover da Vinci:
- The benefits of robotic-assisted surgery
- How da Vinci® Prostatectomy compares to other treatment options
- Whether you are a candidate for da Vinci® Surgery
- Frequently asked questions (FAQs) about robotic-assisted surgery
- Multimedia, including videos, webcasts, podcasts and online patient seminars
- "General Information about Prostate Cancer," National Cancer Institute, www.cancer.gov.
- "Prostate Cancer: Guideline for the Management of Clinically Localized Prostate Cancer":2007 Update. American Urologic Association.
- "What are the Key Statistics About Prostate Cancer?", National Cancer Institute, www.cancer.gov.
- American Cancer Society 2008 Cancer Facts and Figures
- "The Prostate Cancer Outcomes Study: Fact Sheet," National Cancer Institute, www.cancer.gov.
- Gleason score: A system of grading prostate cancer tissue based on how it looks under a microscope. Gleason scores range from 2 to 10 and indicate how likely it is that a tumor will spread. National Cancer Institute, http://www.cancer.gov
- Prostate Cancer Clinical Guideline Update Panel. Guideline for the management of clinically localized prostate cancer: 2007 update. Linthicum (MD): American Urological Association Education and Research, Inc.; 2007. 82 p.
- King CR, Patterns of Prostate Cancer Biopsy Grading: Trends and Clinical Implications. Int J. Cancer (Radiat. Oncol. Invest): 90,305-311(2000).
- Di Blasio, C. J., A. C. Rhee, et al. Predicting clinical end points: treatment nomograms in prostate cancer. Semin Oncol. 2005; 30(5):567-86.
- Carlucci JR, Nabizada-Pace F, Samadi DB. Organ-confined prostate cancer and the emergence of robotic prostatectomy: What primary care physicians and geriatricians need to know. Geriatrics. 2009; 64(2):8-14.
- Tewari A, Raman JD, Chang P, Rao S, Divine G, Menon M.Long-term survival probability in men with clinically localized prostate cancer treated either conservatively or with definitive treatment (radiotherapy or radical prostatectomy). Urology. 2006 Dec; 68(6):1268-74.
- Zelefsky M, Chan H, Hunt M, Yamada Y, Shippy A, Amols H. Long-term outcome of high dose intensity modulated radiation therapy for patients with clinically localized prostate cancer. journal of urology.2006; 176 (4): 1415-1419
- Merrick G. Erectile function after prostate brachytherapy. Int J Radiat Oncol Biol Phys. 2005 Jun; 62(2): 437-47
- "Detailed Guide: Prostate Cancer - Cryosurgery," American Cancer Society, www.cancer.org.
- "Hormone (Androgen Deprivation) Therapy," American Cancer Society, www.cancer.org.
- Benjamin J. Challacombe, Declan G. Murphy, Rhana Zakri and Declan J. Cahill, The Urology Centre, Guy's and St Thomas' NHS Foundation Trust, London, UK, Accepted for publication 21 October 2008
- "Prostate Cancer Treatment: Treatment Option Overview," National Cancer Institute, www.cancer.gov.
Prostate Cancer Causes and Risk Factors
The causes of prostate cancer, as with other cancers, are broad and complex. There is no single perspective on what causes prostate cancer. There are, however, certain factors that are associated with an increased risk of developing prostate cancer.
Age & Genetics
What is known is that prostate cancer is somewhat rare in men under 50 years old, with the risk of developing prostate cancer increasing thereafter. By the time they are 80, more than half of all men will have some cancerous growth, which may or may not require treatment.
Prostate cancer seems to run in some families, suggesting an inherited or genetic factor. Having a father or brother with prostate cancer doubles a man's risk of developing this disease. The risk is even higher for men with several affected relatives, particularly if their relatives were young at the time of diagnosis. Scientists have identified several inherited genes that seem to increase prostate cancer risk.
Some inherited genes increase risk for more than one type of cancer. For example, inherited mutations of the BRCA1 or BRCA2 genes are the reason that breast and ovarian cancers are much more common in some families. The presence of these gene mutations also increases prostate cancer risk. But they are responsible for a very small percentage of prostate cancer cases.
Ethnic origin appears to play a part: men of African heritage seem to be at highest risk, and men of Asian descent are the lowest.
Diet & Lifestyle
Lifestyle choices, diet and exposure to environmental toxins are thought to play a part in the development and speed of prostate cancer.
Diets high in red meat, calcium (dairy products) and bad cholesterol (LDL) are thought to significantly increase prostate cancer risk. Diets high in grain carbohydrates can also affect insulin levels, which may result in obesity. Combined with dietary contributors towards obesity, a lifestyle with little exercise may also lead to development of prostate cancer. Men with a body mass index (BMI) of 32.5 or higher are 30% more likely to die from prostate cancer, while men with a BMI of 35 are 60% more likely to have a recurrence of prostate cancer in 3 years.
Diets that are rich in raw foods and vegetables are known to help prevent prostate cancer. Antioxidant foods help reduce "free radicals" in the body, which damage cell structure and may be a trigger for cancer development. Some common antioxidants include lycopene (found in tomatoes), pomegranate, mangosteen, wheatgrass and seabuckthorn, though the field of antioxidant discovery and research is ever-changing.
There is also research suggesting dietary or supplemented sources of omega 3 and 6 fatty acids, found predominantly in fish, can help prevent cancer, as well as having positive effects on the brain and cardiovascular function. Additionally, supplementation of selenium, vitamin D and vitamin E are thought to be beneficial in preventing prostate cancer as they can lower PSA levels and inhibit tumor growth.
About the Prostate
The prostate gland, a key part of the male reproductive system, is linked closely with the urinary system. It is a small gland that secretes much of the liquid portion of semen, the milky fluid that transports sperm through the penis during ejaculation.1
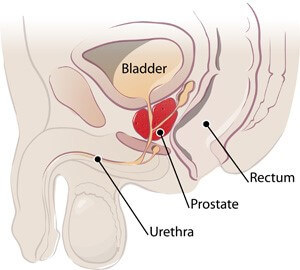
The prostate is located just beneath the bladder, where urine is stored, and in front of the rectum. It encircles, like a donut, a section of the urethra. The urethra is the tube that carries urine from the bladder out through the penis. During ejaculation, semen is secreted by the prostate through small pores of the urethra's walls.2
The prostate is made up of three lobes encased in an outer covering, or capsule. It is flanked on either side by the seminal vesicles, a pair of pouch-like glands that contribute secretions to the semen. Next to the seminal vesicles run the two vas deferens, tubes that carry sperm from the testicles. The testicles, in addition to manufacturing sperm, produce testosterone, a male sex hormone that controls the prostate's growth and function.3
Male hormones cause the prostate gland to develop in the fetus. The prostate continues to grow as a boy progresses to manhood. If male hormone levels are low, the prostate gland will not grow to full size. In older men, the part of the prostate around the urethra often persists in growing. This causes BPH (benign prostatic hyperplasia), which can result in urination problems.4
- "General Information About Prostate Cancer," National Cancer Institute, www.cancer.gov.
- "The Prostate," National Cancer Institute, www.cancer.gov.
- "General Information About Prostate Cancer," National Cancer Institute, www.cancer.gov.
- "What is Prostate Cancer," American Cancer Society, www.cancer.org.
Symptoms of Prostate Cancer
Early prostate cancer usually causes no symptoms and is found by a PSA (prostate-specific antigen) test and/or DRE (digital rectal exam). Some advanced prostate cancers can slow or weaken your urinary stream or make you need to urinate more often. Non-cancerous diseases of the prostate, such as BPH (benign prostatic hyperplasia) often cause these symptoms.
If the prostate cancer is advanced, you might also develop hematuria (blood in your urine) or impotence (difficulty having an erection). Pain in your pelvic bone, spine, hips or ribs is also possible, as advanced prostate cancer commonly spreads to the bones. Other diseases, however, can also cause these same symptoms.
When symptoms do occur, they may include:
- Frequent urination, especially at night
- Inability to urinate
- Trouble starting or holding back urination
- A weak or interrupted flow of urine
- Painful or burning urination
- Blood in the urine or semen
- Painful ejaculation
- Frequent pain in the lower back, hips or upper thighs
For more information on diagnosis, consult the section on Screening & Testing.
Prostate Cancer Growth
Origins in Glandular Cells
Although several other cell types are found in the prostate, over 99% of prostate cancers develop from glandular cells. Glandular cells produce the seminal fluid that is secreted by the prostate. The medical term for a cancer that starts in glandular cells is adenocarcinoma. Because other types of prostate cancer are so rare, if you have prostate cancer, it is almost certain to be adenocarcinoma.
Varied Growth
Most prostate cancers grow very slowly. Autopsy studies show that many older men who died of other diseases also had prostate cancer that neither they nor their doctors were aware of. Some prostate cancers, however, can grow and spread quickly. Even with the latest methods, it is difficult to tell which cancers may become life threatening and which likely do not require treatment.
Changes in Prostate Gland Cells - PIN
Some doctors believe that prostate cancer begins with a condition called prostatic intraepithelial neoplasia (PIN). PIN begins to appear in men in their 20s. Almost 50% of men have PIN by the time they reach 50. In this condition there are changes in the microscopic appearance (size, shape, etc.) of prostate gland cells. These changes are classified as either low-grade, meaning they appear almost normal, or high-grade, meaning they look abnormal. If you have been diagnosed with a high grade PIN on a prostate biopsy, there is a 30% to 50% chance that cancer is also present within your prostate. For this reason, men diagnosed with high-grade PIN are watched carefully and have periodic prostate biopsies.1
- American Cancer Society, What Is Prostate Cancer?
Screening and Testing for Prostate Cancer
There is no standard or routine screening test for prostate cancer. Some screening tests are used because they have been shown to be helpful both in finding cancers early and decreasing the chance of dying from these cancers. Other tests are effective in detecting cancer in some cases, though their efficacy in actually decreasing the risk of death from cancer has yet to be proven.
Scientists study screening tests to find those with the fewest risks and most benefits. Cancer screening trials also are meant to show whether early detection decreases a person's chance of dying from the disease. For some types of cancer, finding and treating the disease at an early stage may result in a better chance of recovery.
Tests to detect prostate cancer include:
1. Digital Rectal Exam (DRE)
During a DRE, the doctor or nurse inserts a lubricated, gloved finger into the lower part of the rectum to feel the prostate for lumps or anything else that seems unusual.
2. Prostate-Specific Antigen (PSA) Test
This test measures the level of PSA in the blood. PSA is a substance made mostly by the prostate that may be found in an increased amount in the blood of men who have prostate cancer. The level of PSA may also be high in men who have an infection or inflammation of the prostate or benign prostatic hyperplasia (enlargement of the prostate gland).
Scientists are studying the combination of PSA testing and using a digital rectal exam as a way to get more accurate results from screening tests. Some cancers never cause symptoms or become life-threatening, but if found by a screening test, the cancer may be treated. It is not known if treatment of these cancers would extend life longer than if no treatment were given, and treatments for cancer may have serious side effects. Follow-up tests, such as a biopsy, may also be done to diagnose cancer.
3. Transrectal Ultrasound (TRUS)
Transrectal ultrasound uses sound waves to make an image of the prostate on a video screen. For this test, a small probe is placed in the rectum. It gives off sound waves, which enter the prostate and create echoes that are picked up by the probe. A computer turns the pattern of echoes into a black and white image of the prostate. The procedure takes only a few minutes and is done in a doctor's office or outpatient clinic. You will feel some pressure when the TRUS probe is placed in your rectum, but it is usually not painful.
4. Biopsy
A biopsy is a procedure in which a sample of tissue is removed and then examined under a microscope. The doctor will use transrectal ultrasound (TRUS) for guidance and insert a narrow needle through the wall of your rectum into several areas of your prostate gland. The needle then removes a cylinder of tissue, usually about 1/2-inch long and 1/16-inch across, that is sent to the laboratory to see if cancer is present.
5. Grading
Healthy prostate cells are uniform in size and shape, neatly arranged in the patterns of a normal gland. As cancer spreads, cells lose their uniform appearance. They change from normal, well-differentiated tissues to more disorganized, poorly differentiated tissue. Eventually, a tumor develops. If your biopsy shows the presence of prostate cancer, the pathologist assigns each tissue sample a grade, indicating how far the cells have traveled along the path from normal to abnormal.
6. Staging
The process used to find out if cancer has spread within the prostate or to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment.
Stages of Prostate Cancer
A staging system is a standardized system of indicating the extent to which a cancer has spread. Staging describes the extent or severity of an individual's cancer based on the size of the original (primary) tumor and the extent to which it has spread within the body. While there are several different staging systems for prostate cancer, the most widely used system in the United States is called the TNM System. It is also known as the Staging System of the American Joint Committee on Cancer (AJCC).1
General Information on Staging
Staging is based on knowledge of the manner in which cancer develops. Cancer cells divide and grow to form a mass of tissue called a tumor. As tumor growth progresses, it can invade nearby organs and tissues. Cancer cells may also break away from the tumor, entering the bloodstream or lymphatic system. By moving through the bloodstream or lymphatic system, cancer can spread from the primary site to form new tumors in other organs. The spread of cancer is called metastasis.2
Purpose of Staging
Staging aids the cancer diagnosis and treatment process in significant ways:
- Staging helps doctors in effectively planning a patient's treatment.
- The stage can be used to estimate a patient's prognosis (likely outcome or course of the disease).
- Knowing the stage aids in identifying clinical trials (research studies) that may be suitable for a particular patient.3
Staging helps researchers and health care providers exchange information about patients, providing a common language for diagnosis, treatment and clinical trials.
Tests to Determine Prostate Cancer Stage
The following tests and procedures may be used in the staging process for prostate cancer:
| TEST/PROCEDURE | EXPLANATION |
|---|---|
|
Radionuclide bone scan |
A procedure to check if there are rapidly dividing cells, such as cancer cells, in the bone. A very small amount of radioactive material is injected into a vein and travels through the bloodstream. The radioactive material collects in the bones and is detected by a scanner.4 |
|
MRI (magnetic resonance imaging) |
A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. This procedure is also called nuclear magnetic resonance imaging (NMRI).5 |
|
Pelvic lymphadenectomy |
A surgical procedure to remove the lymph nodes in the pelvis. A pathologist views the tissue under a microscope to look for cancer cells.6 |
|
CT scan (CAT scan) |
A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.7 |
|
Seminal vesicle biopsy |
The removal of fluid from the seminal vesicles (glands that produce semen) using a needle. A pathologist views the fluid under a microscope to find out if cancer is present.8 |
The results of these tests are viewed together with the results of the original tumor biopsy to determine the prostate cancer stage.
Staging Prostate Cancer Using the TNM System
The TNM System describes the extent of the primary tumor (T stage), whether the cancer has spread to nearby lymph nodes (N stage), and the absence or presence of distant metastasis (M stage). The TNM System has been accepted by the International Union Against Cancer (IUAC) and the American Joint Committee on Cancer (AJCC).9 The stages described below are based on the most recent version of the AJCC staging manual. The clinical stage is based on your tests before surgery, such as your PSA results and your doctor's assessment of the cancer from the DRE. If you have surgery, your doctors can determine the pathologic stage, based on the surgery and examination of the removed tissue. There are 4 categories for describing the prostate tumor's (T) stage, ranging from T1 to T4.10
| STAGE | EXPLANATION |
|---|---|
|
T1 |
Your doctor can't feel the tumor or see it with imaging such as transrectal ultrasound. |
|
T1a |
The cancer is found incidentally during a transurethral resection (often abbreviated as TURP) for benign prostatic enlargement. Cancer is present in less than 5% of the tissue removed. |
|
T1b |
The cancer is found after TURP but is present in more than 5% of the tissue removed. |
|
T1c |
The cancer is found by needle biopsy that was done because of an elevated PSA. |
|
T2 |
Your doctor can feel the cancer when a digital rectal exam (DRE) is done, but it still appears to be confined to the prostate gland. |
|
T2a |
The cancer is in one half or less of only one side (left or right) of your prostate. |
|
T2b |
The cancer is in more than half of only one side (left or right) of your prostate. |
|
T2c |
The cancer is in both sides of your prostate. |
|
T3 |
The cancer has begun to spread outside your prostate and may involve the seminal vesicles. |
|
T3a |
The cancer extends outside the prostate but not to the seminal vesicles.T3b: The cancer has spread to the seminal vesicles. |
|
T4 |
The cancer has spread to tissues next to your prostate (other than the seminal vesicles), such as your bladder's sphincter (muscles that help control urination), your rectum, and/or the wall of your pelvis. |
Stage Grouping
For many cancers, TNM combinations correspond to one of five stages. Once the T, N, and M categories have been determined, this information is combined, along with the Gleason score, in a process called stage grouping. The overall stage is expressed in Roman numerals from I (the least advanced) to IV (the most advanced).11 This is done to help determine treatment options and the outlook for survival or cure. The following graphics, reproduced courtesy of the National Cancer Institute, show the urologic organs and prostate cancer stages.12
STAGE I
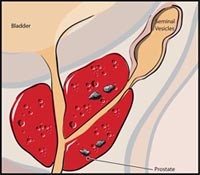
In stage I, cancer is found in the prostate only. It cannot be felt during a digital rectal exam (DRE) and is not visible by imaging. It is usually found accidentally during surgery for other reasons, such as benign prostatic hyperplasia. Stage I prostate cancer may also be called stage A1 prostate cancer.13
STAGE II
In stage II, cancer is more advanced than in stage I, but has not spread outside the prostate. Stage II prostate cancer may also be called stage A2, stage B1, or stage B2 prostate cancer.14
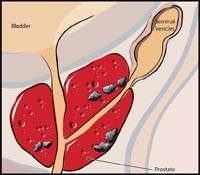
STAGE III
In stage III, cancer has spread beyond the outer layer of the prostate to nearby tissues. Cancer may be found in the seminal vesicles. Stage III prostate cancer may also be called stage C prostate cancer.15
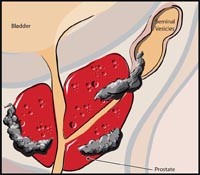
STAGE IV
In stage IV, cancer has metastasized (spread) to lymph nodes near or far from the prostate or to other parts of the body, such as the bladder, rectum, bones, liver, or lungs. Metastatic prostate cancer often spreads to the bones. Stage IV prostate cancer may also be called stage D1 or stage D2 prostate cancer.16
- "Staging: Questions and Answers," National Cancer Institute. www.cancer.gov.
- Ibid.
- Ibid.
- "How is Prostate Cancer Staged?," American Cancer Society, www.cancer.org.
- Ibid.
- Ibid.
- Ibid.
- Ibid.
- "Staging: Questions and Answers," National Cancer Institute. www.cancer.gov.
- "How is Prostate Cancer Staged?," American Cancer Society, www.cancer.org.
- Ibid.
- "Stages of Prostate Cancer," National Cancer Institute. www.cancer.gov.
- Ibid.
- Ibid.
- Ibid.
- Ibid.
Other Treatment Options for Prostate Cancer
In addition to prostatectomy (removal of the prostate) and radiation therapy, a few additional treatment approaches for prostate cancer exist:
- Watchful Waiting
- Hormone Therapy
- Cryosurgery
Watchful Waiting
Watchful waiting, or active surveillance, is based on the premise that some cases of localized prostate cancers may advance so slowly that they are unlikely to cause men - especially older men with a short life expectancy - any problems during their lifetimes. Some men who opt for watchful waiting have no active treatment unless symptoms appear. They are often asked to schedule regular medical checkups and to report any new symptoms to the doctor immediately.
Watchful waiting has the obvious advantage of sparing a man with clinically localized cancer, who typically has no symptoms, the pain and possible side effects of surgery or radiation. On the minus side, watchful waiting risks decreasing the chance to control a disease before it spreads, or postponing treatment to an age when it may be more difficult to tolerate. Of course, treatments may also improve over time if watchful waiting is chosen. Another potential disadvantage is anxiety; some men don't want the worry of living with an untreated cancer.
Patients should educate themselves on the risks vs. benefits of not initiating definitive treatments for prostate cancer, and discuss the option of watchful waiting with their doctor.
Hormone Therapy
Hormone therapy (androgen deprivation therapy) may be used in conjunction with other treatments or alone as a primary treatment. Hormone therapy may act to halt or slow the growth of prostate cancer, and it is often used in men with advanced disease. A variety of hormonal drugs can produce a medical castration by cutting off supplies of male hormones. Female hormones (estrogens) block the release and activity of testosterone. Antiandrogens block the activity of any androgens circulating in the blood. Still another type of hormone, taken as periodic injections, prevents the brain from signaling the testicles to produce androgens.
Hormone therapy has the potential to cause a number of side effects including impotence. Men should discuss the potential benefits and side effects of hormone therapy with their doctors.
Cryosurgery
Cryosurgery uses liquid nitrogen to freeze and kill prostate cancer cells. Guided by ultrasound, the doctor places needles in pre-selected locations in the prostate gland. The needle tracks are dilated for the thin metal cryo probes to be inserted through the skin of the perineum into the prostate. Liquid nitrogen in the cryo probes forms an ice ball that freezes the prostate cancer cells; as the cells thaw, they rupture. The procedure takes about two hours, requires anesthesia (either general or spinal), and requires one or two days in the hospital.
During cryosurgery, a warming catheter inserted through the penis protects the urethra, and incontinence is seldom a problem. However, the overlying nerve bundles usually freeze, so most men become impotent.
The appearance of prostate tissue in ultrasound images changes when it is frozen. To be sure enough prostate tissue is destroyed without too much damage to nearby tissues, the surgeon carefully watches these images during the procedure. But compared with surgery or radiation therapy, doctors know far less about the long-term effectiveness of cryosurgery.
Current techniques using ultrasound guidance and precise temperature monitoring have only been available for a few years. Outcomes of long-term (10- to 15-year) follow-up must still be collected and analyzed. For this reason, most doctors do not include cryosurgery among the options they routinely consider for initial treatment of prostate cancer.
In This Section:
Our Locations
12411 Biscayne Boulevard
North Miami, FL 33181
Phone: (305) 575-2771
Get Directions